
Definition and Etiology:

Rotator cuff tendonopathy is a degenerative condition that affects one or more of the rotator cuff tendons in the shoulder. Studies suggest that it is probably the most common cause of shoulder pain among athletes and the more sedentary population alike. It is estimated that about 30% of the general population experience shoulder pain in their lives and up to 50% of that group are experiencing at least one episode of shoulder pain annually! Even more concerning is that 54% of people with shoulder pain report that their symptoms remain chronic after three years of self-management and that the condition has "changed their habits and lifestyle."
Wait - what happened to the diagnosis: "Rotator Cuff Tendonitis?"
Over the past few years, the medical world has reorganized its thoughts on this diagnosis, and many healthcare professionals (myself included) have upgraded their terminology. More recent imaging studies have shown that no matter the acuteness (recentness) of the injury, with this condition there isn't likely to be much inflammation (the "-itis") around the tendons themselves. Rather, the pain is caused by degeneration and fraying of the rotator cuff tendons, the change in forces on the remaining tissue and the irritation of the tendons gliding in their protective sheath.
The new terminology also brings attention to the increased risk of future tear that underlies this condition. As the condition progresses and more fibers degenerate, the intrinsic strength of the remaining tendon is decreased. What this means is that people with this type of shoulder pain (acute or chronic) are at an increased risk of a rotator cuff tear. The part that I want you to understand is that often, with chronic rotator cuff tendonopathy, the actual tear occurs with a small force. Daily activities like pulling open a heavy door, lifting a pot out of the cabinet with one hand or reaching into the back seat of the car for your bag could be enough to tear the remaining tendon(s). This "small" mechanism of injury is connected to most rotator cuff tears that I treat in the clinic!
What causes RTC tendonopathy?
There are many possible causes, both involving acute trauma and chronic deficits. Some examples include:
- Trauma and incomplete healing after the injury.
- Keeping the arm in the same position for a prolonged period of time, especially overhead positions (such as prolonged hanging, handstand holds/training, one-arm supports, etc).
- Repetitive activities with the arm (could be work or recreational)
- Heavy lifting (usually repetitive or with poor technique)
- Weight bearing on the same arm repetitively. For the average population - this means sleeping or leaning on the same arm. In gymnasts/acrobats/yogis, this could include relying on one arm to do a lever, a single-arm handstand, or a single-arm hang on the fabrics.
- Placing force through the arm in an overhead position (velocity and intensity play a factor).
- Poor coordination/weakness of the shoulder muscles during movement. Medically, this is known as poor scapulothoracic rhythm. Basically, the shoulder blade and the humerus (upper-arm bone) do not move in sync and the forces on the rotator cuff are increased.
- Often chronic shoulder "impingement" is cited as a cause. Shoulder impingement is defined as "the pinching of the subacromial structures, such as the rotator cuff, bursa, and surrounding nerves/vasculature, between the humeral head and acromium with movement." After extensive personal and professional experience and study, I would argue that impingement is caused primarily by poor glenohumeral mechanics. So basically - see the above bullet point.
- Poor posture (through the thorax, shoulders, and neck)
- Increasing age. Studies show that as we age, this tendon weakens/degenerates, making it more likely to see a symptomatic tendonopathy.
- And yes, general overuse (a sudden increase in training or the addition of a new skill) is no doubt a cause.
Symptoms of RTC tendonopathy:
Generally, pain occurs with overhead activities and lifting your arm to the side.

- Pain is most often in the back/top of the shoulder and may radiate to the side of the arm (traditionally the lateral/posterior aspect). The pain is described as a "dull, aching feeling" and does not feel hot/electric. Note: this pain ALWAYS stops before the elbow. If the pain travels beyond the elbow, this may indicate a pinched nerve or more serious pathology.
- The pain may be worst at the beginning of an activity and then "ease off" as you warm-up. This is because the tendon and muscles get more circulation, any small amount of inflammation is cleared, and the remaining healthy tendon has better blood supply/mobility. Often though, there will be an increase in your pain toward the end of or after the activity. This "after" pain can last into the next day and can "keep you up that night."
- There may also be pain with lowering the shoulder from a raised position.
- Sleeping/laying on the affected side may be painful.
Initially, this pain may be mild and occur only with certain movements of the arm. Over time, pain may be present at rest or at night. This constant "toothache" type pain is indicative of progressing severity of the condition.
As the pathology progresses, weakness can develop and sometimes a secondary loss of motion is apparent. Many people with a chronic tendonopathy lose the ability to raise the arm over the head (above 90 degrees). The shoulder will be stiff at rest and the skin around the shoulder will become tender to palpate (massage/touch).
Treatment/Prevention for Rotator Cuff Tendonopathy:
As the condition has MANY causes, treating the injury at home on your own often leaves the problem unresolved. That said, I've got some things to try before you head to your favorite local physical therapist for a professional assessment.
Change your posture:
Without going into the detailed specifics of posture (that's for another post), a quick screen and change in yours can make a world of difference for your rotator cuff. This is because the scapula (shoulder blade) glides along the back of the thoracic spine/ribs. If you have a desk job or you typically slouch, this changes the shape of the surface the scapula moves on. A rounded posture will cause it to tip forward more, and make things like upward rotation (essential with raising the arm) more limited. When this happens, the stress/strain on the rotator cuff increases - and the chance of tendonopathy goes up.
Good posture puts the neck, head, shoulders, and thorax in the ideal position for muscular efficiency. It also ensures that the weight is distributed correctly and that the forces placed on each structure are tolerated.

The head is aligned and looking straight ahead with the ear over the lateral shoulder. The arms are relaxed at the side and the weight falls through the hips, just behind the knees, and over the balls of the feet. There is also even weight on both feet.
To improve your posture, focus on sitting/standing tall with the shoulders back and the chest open. Allow the arms to hang (don't shrug up the shoulders at the neck) and keep the abdominals engaged and the belly flat.
Drink enough water:
This seems like an obvious healthy choice, but several studies have linked dehydration (either through decreased water consumption or increased alcohol consumption) to decreased strength/health of the rotator cuff tendons. While the mechanisms associated with dehydration are more complex than needed for this article, the simple summary is that better hydration has been linked to improved circulation, improved nutrient digestion/absorption and improved tissue texture/health.
Eat enough protein:
It's no secret that good protein intake is an essential part of muscle health and overall fitness. While the source of the protein (vegetable/animal) is for you to decide, the amount should reflect your fitness goals and current lifestyle. If you're training and increasing activity (either for recreation or in the hope of improving your current rotator cuff health), being protein deficient will slow the process and increase your risk of injury.
While I leave the specific calculations to the professional nutritionists, a healthy suggestion for your specific needs comes from the Dietary Reference Intake (DRI). The DRI suggests 0.8 grams of protein per kilogram of body weight, or 0.36 grams per pound. This amounts to: 56 grams per day for the average sedentary man. 46 grams per day for the average sedentary woman. If you're active and building muscle just know that you may need more!
Rest and ice:
While I'm certain that I'll hear back on this, my experience has me firmly believing in ice and rest when you have a sudden flare in rotator cuff symptoms. Rest and ice are just two tools in the "home remedy" toolbox that you might consider in your quest for a healthy RTC.
Rest: I know, you've got a show/meet/big thing coming up, but ultimately this isn't up to you. If you're having these symptoms, your rotator cuff is telling you that there is a problem. Initially, try reducing the number of skill/routine repetitions and focus on drills to strengthen the body and core (conditioning works great as long as it's not over-dosed). If that's not enough and after 1-2 weeks you're still having pain, STOP the offending activity for a few days. Then re-introduce it on a LIMITED basis (2-3 reps a practice and build back up).
Ice: This is a must! After ANY activity that uses the arm or causes pain, sit with ice on it for 10-15 minutes. (and this can include even the non-athletic pursuits of housework and personal hygiene). While the goal of icing isn't as simple as decreasing inflammation, it does help "reboot" the circulatory cycle bydecreasing the flow of blood to that area (the arterial vasculature narrows in response to cold) and giving the lymphatic and venous system a chance to pull out some inflammation. Once the tissue warms after removal, new blood flow with new nutrients are brought to the area and muscle growth/healing can continue. Ice also cools the nerves down and numbs them (by impeding the pain signal up the nerve). As a nerve cools down, it becomes less effective at sending signals. The nerve that carries pain also carries temperature - and it can't carry both at the same time. (This is known as the "Gate Theory of Pain." Think of 495 at rush hour. All the cars want to go, but they can't all fit.) Since temperature is the faster of the two signals, pain has to sit this one out. This allows the muscles to relax (since the brain isn't telling them to reflexively tighten) and helps decrease pain even after the ice is removed.
Stretching/postural exercises:
Now that we've got the treatment started, the next step in the process is stretching and getting the scapular muscles strong enough to efficiently improve scapulothoracic rhythm. Even though it's the tendon that is irritated/degenerating, the true cause of the condition is the musculature - so that's what we have to re-educate. There are many ways to go about this, but I recommend starting with the basics and working up. The focus in the beginning should be on stretching out the anterior shoulder muscles (pectorals, biceps, and anterior deltoid) and strengthening the posterior shoulder and postural muscles (rhomboid, teres minor, infraspinatus, middle, and lower trap). This will help to put the rotator cuff in the ideal position, and also help to improve scapulothoracic rhythm.
Below are some basic recommendations for those at the introductory level. This is only meant as a suggested starting point - there are dozens of ways to strengthen the rotator cuff and realistically, a good physical therapist or personal trainer can tailor your exercises to meet your needs! (Also - check back on this site or our Facebook page for other posts with more exercise ideas.)
Doorway Stretch:
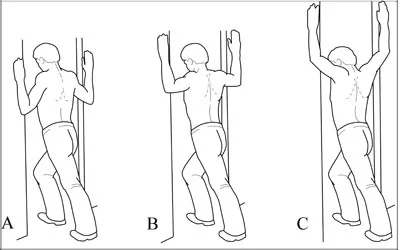
*Note - look straight ahead (the photo shows poor head position)
Standing in a doorway, place your arms on the frame (the shown positions A, B, and C all stretch a different portion of the pectorals). With one leg in front, step through while keeping your head and chest up. You should feel a stretch across your chest and into the front of your arms. Hold for 30 seconds. Perform 3-4 times a day.
Posterior Capsule Stretch:

Grab the back of the arm and pull it across the chest until a stretch is felt in the back of the shoulder. Hold for 30 seconds. Do 3-4 times a day.
Posterior Shoulder Rolls:

Shrug the shoulders up and backward and then relax down and forward. The goal is a backward circling motion. Do 10-20 times, several times a day (while at the computer, sitting in a long meeting, etc).
Shoulder extension stretch:

Standing, slowly bring the arms back and squeeze the shoulder blades together. You should feel a stretch across the chest and muscle contraction between the shoulder blades (postural strengthening). Hold for 10-15 seconds. Do 5-10 times, 1-2 times a day.
Prone YTWL

Laying on your stomach, raise the arms out to the side and make a "Y" a "T" a "W" and an "L." As you lift, focus on squeezing the scapula together (not up towards the neck). Try this exercise with the thumbs pointing up and with the palms flat (facing the floor) as the different position targets different muscles. Do 5-8 reps of all 4, once a day (or every-other day).
Summary:
- Rotator Cuff Tendoopthy is degenerative condition of the rotator cuff tendons in the shoulder.
- It can be caused by trauma, overuse, poor posture, repetitive overhead motion, and poor scapulothoracic rhythm (muscle weakness and poor coordination of the scapula and humerus with arm movement).
- Treatment involves: rest, ice, stretching, and strengthening. A focus on good resting posture is also important.
- As the causes and condition is complex, treatment works best when you consult with a physical therapist. There is truly no "one-size fits all" approach to rehabilitating this condition!
References:
- Chris Littlewood, Stephen May and Stephen Walters, (2013) Systematic Reviews of the Effectiveness of Conservative Interventions for Rotator Cuff Tendinopathy, review.
- Cohen R, William G (1998) Impingement syndrome and rotator cuff disease as repetitive motion disorder. Clin Orthop 351:95–100.
- Dutton, M. (2008). Orthopaedic: Examination, evaluation, and intervention (2nd ed.). New York: The McGraw-Hill Companies, Inc.
- Jia X, Petersen SA, Khosravi AH, Almareddi V, Pannirselvam V, McFarland EG. Examination of the shoulder: the past, the present, and the future. J Bone Joint Surg Am. 2009;91:10-8.
- Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med 1998; 26:325-337
- Nitin B. Jain, MD, MSPH1, Reginald Wilcox, PT, Jeffrey N. Katz, MD, MS, and Laurence D. Higgins, MD. Clinical Examination of the Rotator Cuff, manuscript, 5 January 2013.
- Neumann DA. Kinesiology of the musculoskeletal system: Foundations for Physical Rehabilitation.2nd Ed. Elsevier Health Sciences; 2009
- Sahrmann, S. Diagnosis and Treatment of Movement Impairment Systems. (2002) Missouri; Mosby Inc.