
Arguably one of the most injured and dysfunctional muscle groups in the shoulder, the rotator cuff is essential for all shoulder motions.
Review of the anatomy of the Rotator Cuff:
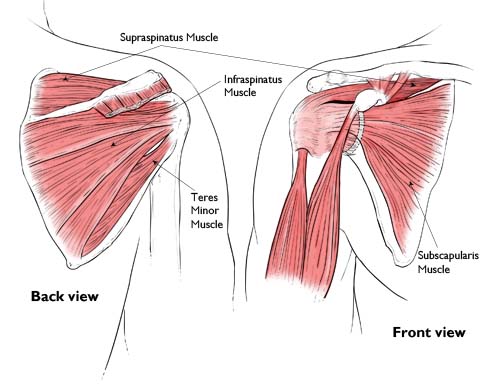
The rotator cuff is composed of four small, short muscles that originate on the scapula and pass around the shoulder where their tendons fuse together and attach on the humerus. Known as the "SITS" muscles, they are:
- Supraspinatus - anchors the humeral head in the glenoid. It is thought to assist with abduction (lateral raising of the shoulder) in the early phase of the motion. It also works to hold the humeral head in position with traction forces (think 10 bags of groceries and only one trip from the car…). Of the four rotator cuff muscles, this is the muscle most often torn.
- Subscapularis - this muscle sits between the shoulder blade and the back of the rib cage (on the anterior surface of the scapula). Its main functions are internal rotation (twisting the arm in) and adduction (bringing the arm tight against your side). It is the largest of the rotator cuff muscles and its actions are assisted by the pectoralis major muscle - and as such, is not as susceptible to injury.
- Infraspinatus - this muscle sits on the back of the scapula (shoulder blade) and below the supraspinatus and scapular spine (that bony ridge you can feel if your reach over your shoulder and touch the top of your shoulder blade. Its main function is external rotation (twisting the arm out) and it assists with extension (bringing the arm back) and horizontal abduction (pulling the arm back at shoulder height). It is much smaller than the subscapularis.
- Teres minor - this muscle sits just inferior to the infraspinatus. It is also an external rotator of the shoulder and assists with extension and horizontal abduction. This muscle is often lumped in with the infraspinatus as it has similar functions.
As a group, these muscles have two main functions:
- Stabilization. These muscles stabilize the joint and help center the humeral head in the glenoid fossa (important in preventing pain and injury). During abduction (lateral elevation) of the arm, the rotator cuff anchors the humeral head, forcing it to pivot while the deltoid contracts to raise the arm. If the deltoid were to work without the rotator cuff, the humeral head would be pulled up and toward the top of the glenoid fossa - causing it to bump into the acromion (tip of the shoulder blade) and making the motion of abduction limited (by a lack of joint space and ultimately pain).
- Coordination. The rotator cuff muscles control rotation of the shoulder and allow for complex movements in almost 360 degrees of motion. When working properly, the rotator cuff allows for precision movements of the scapula, clavicle and humerus such that mobility is unrestricted while stability is maintained.
Injury to the Rotator Cuff:
There are several mechanisms by which the rotator cuff can be injured/damaged. These include:
- Direct trauma: such as a fall or unexpected force through the joint.
- Overuse/repetitive stress: this can include chronic impingement (the acromion slowly saws through the rotator cuff tendon), poor posture and mechanics of the shoulder joint, chronic tendonitis, and even degenerative joint disease (the arthritis and loss of cartilage changes the joint space and increases forces on the cuff).
- Pathologic weakness: Pathologic weakness (such as systemic muscular/joint disease and nerve injury) can make the rotator cuff more susceptible to injury. The rotator cuff is innervated (controlled by the nerves) C5-C6 which exit the neck just under the clavicle. If there is any compression on these nerves, the signals they send to control the rotator cuff can be decreased, and the muscles become functionally weaker. If that's the case, even a small stress can cause a traumatic tear (reaching for a purse, lifting a pot, doing a pull up, etc.) More interesting to note – the most common site for disc herniation/injury in the neck is the C5/C6 segment! This means that many rotator cuff injuries are likely paired with neck problems (so make sure your PT is addressing that in your treatment too).
Acrobatics and the rotator cuff:
Warning: the following contains some complex thinking and is mostly personal theory (so take what you want from it and ignore the rest).
It should come as no surprise that acrobatics, gymnastics and body weight strength training put a huge strain on the rotator cuff. The various body positions required often bias the athlete’s arm and shoulder into positions where the rotator cuff is disadvantaged and forced to contract to stabilize the joint. Even worse, some elements require the rotator cuff to act as a prime mover.
Now, with certain skills/exercises in these sports, the shoulder is required to be a weight bearing joint. (Warning: this is not what it was designed for). There are two types of weight bearing encountered by the shoulder in acrobatics (including gymnastics, aerials and body weight strength training): compression/approximation & traction/distraction. Compression is the traditionally accepted term for weight bearing. Compression can be defined as the force of gravity and weight as they pass through and approximate the bones of the joint (as in a handstand). The term I'm adding as a "weight bearing" activity is traction. In this case, the force is through the joint capsule the ligaments, and the surrounding muscles (rather than the bones of the joint), In the shoulder, arguably the rotator cuff plays a huge role in traction weight bearing - it is the muscular stabilizer!

Bones of the glenohumeral joint (shoulder)
Tiny glenoid with a larger humeral head - designed for mobility not stability.

Bones of the hip joint
Notice the larger joint surfaces and the increased joint congruence when compared with the glenohumeral joint above.
Beyond that, the size of the joint is much larger than that of the glenohumeral joint (2-3x larger in most people) to accommodate the weight bearing requirements of the structure.
Structurally and anatomically, weight bearing is not what the shoulder is primarily designed for.
If you look at the hip, a truly weight bearing joint, the joint congruity (the amount of surface area in contact between the 2 bones of the joint) is very high. This spreads the forces out and gives stability. The hip also has significant musculature (specifically the gluteal muscles and hip rotators) that assist in stabilizing and adding congruity to the joint. This is an evolutionary upgrade - something we took on when we began to walk upright on two legs as our primary means of transport.
This is NOT the case in the shoulder (which was likely downgraded at about the same time in our evolutionary history). It has a very low level of congruity (think tennis ball balanced on a quarter) and is designed for mobility. It also does not have as thick of a joint capsule and has less density and fewer ligaments around it than the hip. Finally, in the hip, the gluteal muscles and the hip rotators are some of the thickest muscles in the body. Their "analogous" structures in the shoulder - the pectorals and the rotator cuff are quite tiny in comparison.
See the dilemma? We acrobats are fighting the evolutionary chain of events and trying to return to the activities of our now far-estranged 4-limb ambulating ancestors. Swinging, standing, jumping, and walking on our hands and arms requires much more of the rotator cuff and the shoulder muscles in general.
Drum roll for some fun structural facts: According to a study published in the Journal of Clinical Sports Medicine, the shoulder capsule (the ligaments surrounding the shoulder) have s tensile strength of 100-180 pounds at full maturity. This means that any force through the joint that exceeds that amount requires the rotator cuff to contract and provide enough force to protect the joint.
Now - think about a giant swing on the uneven bars, a drop into a hang on the aerial silks or even an inlocate on rings. For all you mathematical whizzes out there - combine your body weight with gravity (F = ma) and then add in torque (T = Fd) and factor in some momentum (p = mv) and ta-da! Your rotator cuff just tried to provide enough force to substitute for a cable on the nearest suspension bridge…
With requirements like that, it’s no wonder that rotator cuff injury and dysfunction is more common in overhead athletes and acrobats. It makes consistent strengthening and protection of this muscle group an essential part of and training routine.
References:
Codman EA. The shoulder. Malibar, Florida: R.E. Kreiger; 1934
Jia X, Petersen SA, Khosravi AH, Almareddi V, Pannirselvam V, McFarland EG. Examination of the shoulder: the past, the present, and the future. J Bone Joint Surg Am. 2009;91:10-8.
Sahrmann, S. Diagnosis and Treatment of Movement Impairment Systems. (2002) Missouri; Mosby Inc.